How antiviral pill molnupiravir shot ahead in the COVID drug hunt
The Merck pill, which could become the first oral antiviral COVID treatment, forces the SARS-CoV-2 coronavirus to mutate itself to death.
어떻게 항바이러스제 몰누피라비르가 COVID 마약사냥에서 앞서갔는지
최초의 경구용 항바이러스 COVID 치료제가 될 수 있는 머크 알약은 사스-CoV-2 코로나바이러스가 스스로 변이를 일으켜 죽게 만든다
If authorized, molnupiravir would be the first oral treatment for COVID-19.Credit: Merck & Co Inc/Handout/Reuters
오렌지 실험용 COVID-19 치료제 몰누피라비르 클로즈업 허가를 받으면 몰누피라비르는 COVID-19의 첫 번째 구강 치료가 될 것이다.크레딧: Merck & Co Inc/인출/로이터
The pharmaceutical firm Merck announced last week that an antiviral pill it’s developing can cut hospitalizations and deaths among people with COVID-19 by half. The results haven’t yet been peer reviewed. But if the drug candidate, molnupiravir, is authorized by regulators, it would be the first oral antiviral treatment for COVID-19. By contrast, the other currently authorized drugs must be delivered intravenously or injected.
A pill could make treating patients earlier on in their infection much easier — and more effective. It could also keep hospitals from overflowing, especially in places where vaccination rates are still low, such as many low- and lower-middle-income countries. Molnupiravir was so effective in a phase 3 trial involving COVID-19-positive people at risk of severe illness that clinicians halted enrolment early.
But whether this clinical-trial success story will translate into a global game-changer in the fight against the pandemic isn’t yet clear. Even if lower-income countries can afford the medicine, they might not have the diagnostic capacity to treat patients with molnupiravir early in the course of their illness, when treatment could make a difference.
This week, two Indian drugmakers independently testing generic molnupiravir in people with moderate illness due to COVID-19 sought to end their trials because they saw no “significant efficacy” for the experimental drug, although they plan to continue trials for people with mild illness. Merck’s findings, which were disclosed in a press release and have yet to be pored over by scientists and submitted to regulators for approval, applied to people with mild-to-moderate cases of COVID-19 who were not hospitalized. A spokesperson for Merck points out that moderate COVID-19 cases in India are defined as being more severe than in the United States and involve hospitalization.
Hit early, hit hard
The other therapies on offer against COVID-19, Gilead Science’s antiviral remdesivir and a monoclonal antibody cocktail from biotech firm Regeneron, must be administered intravenously or by injection. That makes it difficult for people to access the therapies before they are sick enough to land in hospital. And remdesivir is approved only for those who are already hospitalized with COVID-19.
Yet it’s better to “hit early, hit hard” with antivirals, says Richard Plemper, a virologist at Georgia State University in Atlanta. The sicker the patient, the less effective the drugs are at treating the illness. A COVID-19 pill, which simply requires a prescription and a trip to the pharmacy once symptoms appear, would make early treatment much easier.
COVID-19 is not the first disease caused by a coronavirus to seriously impact humans. But the 2002–04 severe acute respiratory syndrome (SARS) epidemic fizzled out quickly, and the Middle East respiratory syndrome (MERS) outbreak in 2012 never became widespread — meaning that drugmakers had little incentive to develop antivirals against these diseases.
So when the first cases of COVID-19 emerged in late 2019, “there wasn’t a portfolio of antivirals waiting”, says Saye Khoo, an infectious-disease physician at the University of Liverpool, UK, who has led a clinical trial of molnupiravir.
Initial efforts to find treatments focused on drugs already approved by regulators, and yielded only one winner: dexamethasone, a steroid aimed at dampening an overblown inflammatory response in the sickest people. The FDA has not authorized the drug for this purpose, but it's widely used to treat the sickest people.
제약회사 머크는 지난 주 개발중인 항바이러스제가 COVID-19에 걸린 사람들의 입원과 사망률을 절반으로 줄일 수 있다고 발표했다. 결과는 아직 동료 검토되지 않았다. 그러나 만약 약물 후보인 몰누피라비르가 규제당국의 허가를 받는다면, 이것은 COVID-19에 대한 최초의 경구용 항바이러스 치료제가 될 것이다. 이와는 대조적으로, 현재 허가된 다른 약들은 정맥주사로 전달되거나 주입되어야 한다.
관련 COVID를 물리칠 항바이러스제 경쟁과 다음 대유행
알약은 감염 초기에 환자 치료를 훨씬 쉽고 효과적으로 만들 수 있다. 그것은 또한 병원이 넘쳐나는 것을 막을 수 있는데, 특히 많은 저소득 및 저소득 국가들과 같이 백신 접종률이 여전히 낮은 곳에서는 더욱 그러하다. 몰누피라비르는 중증 질환의 위험에 처한 COVID-19 양성 환자를 대상으로 한 3단계 시험에서 너무 효과적이어서 임상의사들은 등록을 조기에 중단했다.
그러나 이 임상적-재판적 성공 사례가 전염병과의 싸움에서 세계적인 판도를 바꿀 수 있을지는 아직 분명하지 않다. 저소득 국가들이 이 약을 살 여유가 있다고 해도, 그들은 치료가 차이를 만들 수 있는 그들의 병의 과정 초기에 몰누피라비르 환자를 치료할 진단 능력이 없을지도 모른다.
이번 주, 두 명의 인도 제약회사들이 독립적으로 COVID-19로 인해 중간 정도의 질병을 가진 사람들에게서 일반적인 몰누피라비르를 검사했는데, 그들은 가벼운 병을 가진 사람들에 대한 실험을 계속할 계획임에도 불구하고 실험 약물에 대해 "상당한 효능"을 보지 못했기 때문에 그들의 실험을 끝내기 위해 노력했다. Merck의 연구결과는 보도자료를 통해 공개되었고 아직 과학자들에 의해 검토되어 규제당국에 승인을 받기 위해 제출되지 않은 것으로 입원하지 않은 경증에서 중증급 COVID-19 사례를 가진 사람들에게 적용되었다. Merck 대변인은 인도의 보통 COVID-19 사례는 미국보다 더 심각하고 입원이 수반된다고 지적한다.
일찍 치고, 세게 때린다.
COVID-19에 대항하여 제공되는 다른 치료법, 길리어드 사이언스의 항바이러스 렘데시비르와 생명공학 회사인 리제네론의 단일클론 항체 칵테일은 정맥주사 또는 주사를 통해 투여되어야 한다. 이것은 사람들이 병원에 도착할 만큼 아프기 전에 치료법에 접근하는 것을 어렵게 만든다. 그리고 렘데시비르는 이미 COVID-19로 입원한 사람들에게만 승인된다.
관련 코로나바이러스의 획기적인 발전: 덱사메타손은 생명을 구하는 것으로 나타난 첫 번째 약이다.
그러나 항바이러스제를 "일찍 때리고, 심하게 때리는" 것이 낫다고 애틀랜타 조지아 주립대학의 바이러스학자인 리차드 플렘퍼는 말한다. 환자가 아플수록, 그 약은 병을 치료하는 데 효과가 떨어진다. 일단 증상이 나타나면 처방과 약국 방문이 필요한 COVID-19 알약은 조기 치료를 훨씬 쉽게 해줄 것이다.
COVID-19는 인간에게 심각한 영향을 미치는 코로나바이러스에 의한 첫 번째 질병이 아니다. 그러나 2002-04년 중증급성호흡기증후군(SARS) 유행은 빠르게 소멸되었고, 2012년 중동호흡기증후군(MERS) 발발은 널리 퍼지지 않았다. 즉, 제약회사들이 이러한 질병에 대한 항바이러스제를 개발할 동기가 거의 없다는 것을 의미한다.
따라서 2019년 말 COVID-19의 첫 사례가 나타났을 때 "항바이러스 포트폴리오가 기다리고 있지 않았다"고 몰누피라비르 임상 실험을 이끈 영국 리버풀 대학의 전염병 내과의사인 Saye Khoo는 말한다.
규제당국에 의해 이미 승인된 약물에 초점을 맞춘 치료법을 찾기 위한 초기의 노력은 단 한 명의 승자를 내주었다: 가장 아픈 사람들의 부풀려진 염증 반응을 억제하기 위한 스테로이드인 덱사메타손. FDA가 이 약을 허가하지는 않았지만, 가장 아픈 사람들을 치료하기 위해 널리 사용되고 있습니다.
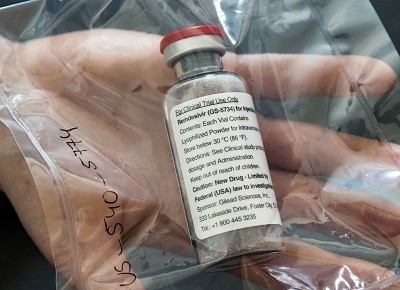
The US Food and Drug Administration has authorized remdesivir, an intravenously administered antiviral, only for use in people hospitalized with COVID-19.Credit: Scott Olson/Getty
But even as researchers scrambled to test approved drugs, pharmaceutical companies and biotechnology firms were scouring their libraries for any compounds with known antiviral activity that might stop the SARS-CoV-2 coronavirus. These broad-acting antivirals weren’t designed specifically to target SARS-CoV-2, but it seemed mechanistically feasible that they could. Unlike with many of the drugs tested early in the pandemic, “there’s a scientific rationale. You understand how they’re working”, says Jay Luly, chief executive of Enanta Pharmaceuticals, a company in Watertown, Massachusetts, that is developing its own COVID-19 antiviral.
So far, Gilead’s remdesivir is the only such drug that has received approval from the US Food and Drug Administration. When used in a hospital setting, its effect is modest. In a phase 3 trial, researchers found that it shortened recovery time by a median of 5 days1. Merck hopes molnupiravir will be next to receive authorization.
Hot pursuit
Molnupiravir began as a possible therapy for Venezuelan equine encephalitis virus at Emory University’s non-profit company DRIVE (Drug Innovation Ventures at Emory) in Atlanta. But in 2015, DRIVE’s chief executive George Painter offered it to a collaborator, virologist Mark Denison at Vanderbilt University in Nashville, Tennessee, to test against coronaviruses. “I was pretty blown away by it,” Denison remembers. He found that it worked against multiple coronaviruses: MERS and mouse hepatitis virus2.
Painter also recruited his collaborator Plemper to test the drug against influenza and respiratory syncytial virus. After the pandemic hit, however, plans changed. DRIVE licensed the compound to Ridgeback Biotherapeutics in Miami, Florida. Plemper, too, pivoted to coronaviruses, and tested the compound in ferrets. It silenced the virus’s ability to replicate, he says, but it also suppressed the virus’s transmission from infected ferrets to uninfected ones3. Merck’s data hint that might also be true in humans: molnupiravir appeared to shorten the duration of SARS-CoV-2’s infectivity in trial participants with the virus.
Molnupiravir, like remdesivir, is a nucleoside analogue, which means it mimics some of the building blocks of RNA. But the compounds work in entirely different ways. When SARS-CoV-2 enters a cell, the virus needs to duplicate its RNA genome to form new viruses. Remdesivir is a ‘chain terminator’. It stops the enzyme that builds these RNA ‘chains’ from adding further links. Molnupiravir, on the other hand, gets incorporated into burgeoning RNA strands and, once inside, wreaks havoc. The compound can shift its configuration, sometimes mimicking the nucleoside cytidine and sometimes mimicking uridine. Those RNA strands become faulty blueprints for the next round of viral genomes. Anywhere the compound gets inserted and that conformational shift happens, a point mutation occurs, Plemper says. When enough mutations accumulate, the viral population collapses. “That is what we term lethal mutagenesis,” he adds. “The virus essentially mutates itself to death.” And because the mutations accumulate randomly, it’s difficult for viruses to evolve resistance to molnupiravir — another plus for the compound.
But the compound’s mutagenic potential in human cells — the possibility that it could incorporate itself into DNA — does raise safety concerns, some researchers say. Merck hasn’t released any detailed safety data yet, but “we’re very comfortable that the drug will be safe if used as intended”, said Daria Hazuda, Merck’s vice-president of infectious-disease discovery and chief science officer, at a press briefing last Friday.
Waiting in the wings
Other antivirals are in the works. Gilead Sciences is developing a pill version of remdesivir. And Denison suspects that if the antiviral were given to people as early as molnupiravir is — when symptoms have only just appeared and viral loads are high — it would be similarly effective. In a study presented at IDWeek, a virtual meeting of infectious-disease specialists and epidemiologists held earlier this month, researchers reported results of administering infusions of remdesivir to people in the early stages of COVID-19 every day for three days. The number of participants in the study was small, but remdesivir appeared to reduce hospitalizations by 87% in people at high risk of developing COVID-19.
Biotech firm Atea Pharmaceuticals in Boston, Massachusetts, also has an antiviral in the works. It was testing a nucleoside analogue against hepatitis C in a clinical study when SARS-CoV-2 emerged. The pandemic paused the trial, so Atea decided to switch its focus to COVID-19. Now it has partnered with Roche in Basel, Switzerland, to develop its compound.
Pfizer, based in New York City, had a bit of a head start too. The company had been developing antivirals against SARS since the early 2000s, but shelved them when the outbreak ebbed. When the COVID-19 pandemic began, “they just blew the dust off”, Luly says. Researchers are currently testing a pill form of a compound that has a mechanism of action similar to those original versions. It is in phase 2/3 trials for treating people who are newly infected.
Global access
An effective oral antiviral would be an incredible asset in the fight against COVID-19, but it’s not yet clear whether molnupiravir will be accessible to all. “Are we going to be in a situation where the price is reasonable in low- and middle-income countries?” asks Rachel Cohen, the North American executive director at the Drugs for Neglected Diseases initiative.
The United States has agreed to purchase 1.7 million courses of molnupiravir for US$1.2 billion, which works out to about $700 per 5-day course. That’s far less than the price of remdesivir or monoclonal antibodies, but still too costly for much of the world. Merck, which is co-developing the compound with Ridgeback, has struck licensing agreements with five Indian manufacturers of generic drugs. Those deals allow the manufacturers to set their own price in India and 100 other low- and lower-middle-income countries.
But even if poorer countries can afford the drug, they might not have the diagnostic capacity to use it properly. If molnupiravir needs to be given in the first five days after symptom onset, “that requires that we are able to actually rapidly diagnose people”, Cohen says. For many developing countries — and even some wealthy ones — “that is actually a huge challenge”.
Clarification 09 October 2021: This story was updated to clarify that the two Indian drugmakers testing a generic version of molnupiravir did so independently of Merck, and to add comments from Merck indicating that moderate cases of COVID-19 in India are defined as being more severe than those in the United States.
References
1.
Beigel, J. H. et al.N. Engl. J. Med.383, 1813-1826 (2020).









댓글목록